Posterior Interosseous Nerve: Neuropathy, Dysfunction, and Posterior Interosseous Nerve Syndrome.
The radial nerve is a major peripheral nerve of the upper extremity that travels down the arm. The terminal branches arise at the level of forearm extensors muscles and become terminal branches of the radial nerve just distal and posterior to the elbow at the supinator muscle. The two terminal branches of the radial nerve divide at the supinator muscle with superficial sensory branches innervating the skin of the dorsal hand and forearm, while the posterior interosseous nerve arises just prior to the superficial head of the supinator. The relationship of the posterior interosseous nerve incarcerated within the supinator muscle is known as Posterior interosseous nerve injury or syndrome. The fascial relationship between the posterior interosseous nerve and the supinator muscle is known as the Arcade of Frohse.
Posterior Interosseous Nerve Syndrome Symptoms
After the nerve passes the level of the elbow it becomes referred to as the deep motor branch of the radial nerve and innervates the forearm extensors muscles excluding the brachioradialis and extensor carpi radialis longus/brevis. The deep branch or the radial is a pure motor nerve with symptoms including weakness of finger extension, pain over the lateral elbow, and area of the radial forearm. The superficial branch of the radial nerve travels over the surface on the supinator and avoiding compression in the tunnel. Therefore, no sensory disturbances are present with the incarcerated posterior interosseous nerve.

")
Entrapment and injury areas for the Posterior Interosseous nerve.
The areas the posterior interosseous nerve becomes injured according to Konjengram.
- Fibrous adhesions anterior radio-humeral joint capsule and the DBRN
- Interaction with the extensor carpi radialis brevis muscle
- Radial recurrent vessels compressing the nerve
- Superior border and inferior borders of the superficial layer of the supinator muscle (arcade of Frohse). Most common entrapment site
- Distal border of supinator as it exits the tunnel to innervate forearm extensor muscles.
It’s important in the NeuroCentric Approach to assess and elevate mechanically derived nerve compression causing ischemia to the nerve, both extra-neural and intra-neural based. Transverse nerve mobilizations of the posterior interosseous nerve are an effective procedure to reduce the mechanical compression of the radial nerve.

Arcade of Frohse: The primary incarcerator of the deep radial nerve in the arm.
The Arcade of Frohse is arch is typically a fibrous connective tissue arch between the two heads of the supinator muscle that radial nerve enters on its path to innervate the deep forearm extensor muscles. The arcade of Fronshe is the primary compression site of the PIN and equates to 76% of posterior interosseous nerve compression injuries to the forearm area. (anania paper).
It’s important to note that the Arcade of Frohse isn’t always a fibrous arcade. Just like many areas of anatomy, there are variations that need to be considered. According to ….there are actually 4 types of connective tissue arcades that exist for the entry point for the radial nerve. These are a pure tendinous arcade, Musulo-tendinous blend arcade, pure muscular arcade, and a membranous arcade. The tendinous arcade is thought to be the primary variation present that becomes thickening and creates mechanical compression of the radial nerve.
A thick tendinous arcade that has become fibrotic is thought to be the primary presentation that creates entrapment of the posterior interosseous nerve. This scenario can be seen on ultrasound by the classic presentation of nerve swelling proximal to impingement and thinning (lack of blood flow) after the area of entrapment by the tendinous arcade.
 Palpation of the Posterior Interosseous Nerve in the Forearm
Palpation of the Posterior Interosseous Nerve in the Forearm
The posterior interosseous nerve and its relationship to the forearm and lateral elbow pain is an important differential diagnosis in the NeuroCentric Approach ™. Conservatively speaking in diagnosis and treatment, it’s vital to accurately be able to palpate an entrapment site of the radial nerve. Therefore knowing the nerve location bases on surgically anatomy research and being able to provide mechanical stress to the nerve with palpation is an extremely important aspect of the exam.
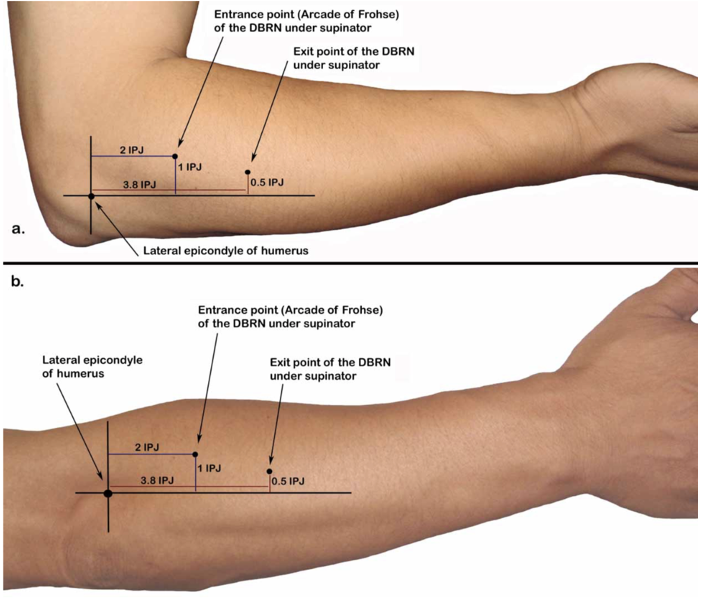
During surgical interventions, it’s important to know the radial nerves’ location bases on superficial landmarks, typical branching patterns, and variations of those branching patterns. Otherwise, significant nerve injury can result.
The interphalangeal joint (IPJ) of the thumb is a helpful clinical tool in finding the Arcade of Frohse and the exit point of the deep radial nerve. Using the IPJ one can accurately and quickly find the relative location of the common entrapment sites of the posterior interosseous nerve and apply an intervention if needed using the Clinical Audit Process with the NeuroCentric Approach (TM).
GET IN TOUCH WITH DR. DEAN
YOU should be able to move the way you’d like to move without experiencing pain. YOU should be able to experience freedom and energy knowing there’s nothing holding back from giving your life 110%. Dr. Dean would like to learn more about your challenges with a quick phone or email before beginning treatment. Contact him today.